
Centre of Recovery Excellence manipulating health information of people who use drugs to undermine their safety
The Alberta government's Crown corporation has published its first study using personal health numbers of people accessing supervised consumption sites. While its findings fail to hold up, it offers a case study of how conflicts of interest and privacy oversight are at a crisis point in Alberta.
"You're only supposed to use the amount of health information that is necessary. Just because you're allowed to get it and disclose it without consent doesn't mean that you should," asserts Dr. Lorian Hardcastle, Associate Professor at the University of Calgary's Faculty of Law. "What is the government saying is the justification for needing personally identified information?"
That reason became clear on March 10, as the Alberta government's new Crown corporation, the Canadian Centre of Recovery Excellence (CoRE), published its first study using individually identifying information of people who use drugs. Minister of Mental Health and Addiction Rick Wilson thanked the CoRE on March 11 for its "rigorous, high-quality research that helps inform responsible and evidence-based addiction policy."
The study, announced on March 10 in a CoRE press release, purports to show that "closing [an] Alberta Overdose Prevention Site led to no increase in overdose deaths and an increase in life-saving treatment." The study made use of the government's mandated collection of personal health numbers (PHNs) at supervised consumption services to make its claims.
Reacting to these press releases, Friends of Medicare executive director Chris Gallaway told Drug Data Decoded that the government appears to be "creating a whole research entity to validate their approach, then saying, 'Oh wow, they validated our approach."
In keeping with Gallaway's concerns around CoRE being used to create propaganda, the study failed to disclose key facts that undermine its claims.
The most critical among these is that CoRE staff were well aware as early as 2024 that PHNs of deceased people were turning up at the sites, indicating that an unknown proportion of people accessing the sites use fake PHNs. Although this limitation throws the entire dataset into question, it was omitted from the study.
The study also failed to contend with – or even cite – the landmark 2024 finding that supervised consumption sites may decrease deaths by up to two-thirds in neighbourhoods that contain them. Documents show the study authors deliberating that study internally, revealing that the authors chose to ignore that finding.
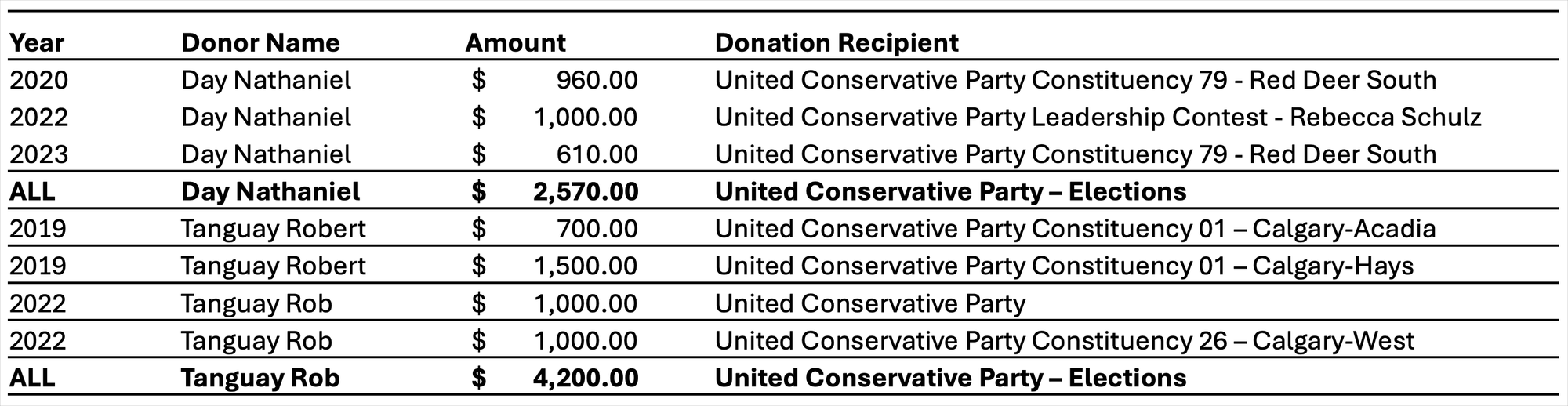
The second key issue, also undisclosed in the study, is that lead author Dr. Nathaniel Day has donated over $2,500 to the United Conservative Party. Study co-author Dr. Rob Tanguay appears to have donated over $4,000 to the UCP and receives undisclosed government funding to the treatment centre he co-founded, Newly Institute.
Tanguay was co-chair of the notorious UCP-appointed 2019 supervised consumption site review that has been used internationally by governments eager to show 'data' supporting site closures. That panel's findings were upended by peer-reviewed criminological and public health analyses. In 2020, Tanguay publicly apologized for his role in the panel.
Meanwhile, despite Day's political support, he served as expert witness for the United Conservative government against Ophelia Black's 2023 injunction lawsuit to preserve her access to regulated hydromorphone. (The government recently renewed its attempt to have Black's injunction overturned.) Day also omitted key internal data and mischaracterized the landmark Toronto study in his 2025 affidavit supporting the Ontario government's closure of sites.
On March 10, Day was asked by Drug Data Decoded to comment on whether his political donations rendered his 2023 expert witness testimony inappropriate. He did not respond.
Another possible conflict of interest arises at the journal in which the study was published. The deputy editor-in-chief of the Addiction journal is a board member and heavy investor in the pharmaceutical company best positioned to benefit from the study's findings, as well as a longtime advisor on Alberta government policy panels. In Alberta, dispensing of Indivior's flagship patented opioid agonist medication, Sublocade, rose from zero to 180 individuals per 100,000 between 2020 and 2025. In this period, methadone dispensing remained flat.
(Drug Data Decoded holds no records indicating Humphreys influenced the study's publication.)

Thirdly, CoRE presents itself in the study as an organization that "receives public funding from the Government of Alberta," claiming that "the funder had no role in the study design, data analysis, interpretation of results, manuscript preparation or the decision to submit this work for publication."
This is misleading, as the CoRE is part of the government, not simply a funding recipient. According to the 2025-28 Ministry business plan, "the Ministry of Mental Health and Addiction is composed of the Department of Mental Health and Addiction, Recovery Alberta, the Canadian Centre of Recovery Excellence (CoRE), and the Mental Health Review Panels."
By definition, the Alberta government had a role in all elements of the study, because ten of the eleven study authors are in the government.
This is not something they've done before. It's not something other places are doing.
-Dr. Lorian Hardcastle, University of Calgary
The Alberta government launched the CoRE in August 2024 alongside Recovery Alberta, the first of several new health care authorities that would fragment 100,000 Alberta Health Services employees.
While Recovery Alberta would receive about 10,000 of those employees, the CoRE would be run by a smaller group with a budget of around $5 million to "find the most effective ways to support recovery ... with the best available information on what works and what does not work."
The CoRE facilitates research projects through an appointed Research Council that approves or denies project applications. The Research Council includes Nathaniel Day, Shelly Vik, Daniel Devoe, and Vanessa Norton – all authors of the CoRE's study on supervised consumption site closures.
As reported by Drug Data Decoded, Day reached out to Vik on January 25, 2025, offering to "join the project team to help" – nine months before the study was submitted to Addiction with Day as lead author.

The CoRE is given unprecedented rights to access individualized health information of people who use drugs using Recovery Alberta clinical data collection. Documents obtained by Drug Data Decoded reveal that on December 20, 2024, a request was sent to Recovery Alberta officials on behalf of CoRE CEO Kym Kaufmann, asking for "de-identified" (anonymous) data concerning My Recovery Plan, navigation centres and supervised consumption sites. The request closed with a note that in the near future, the CoRE would require "identified record level data for these and other relevant datasets."

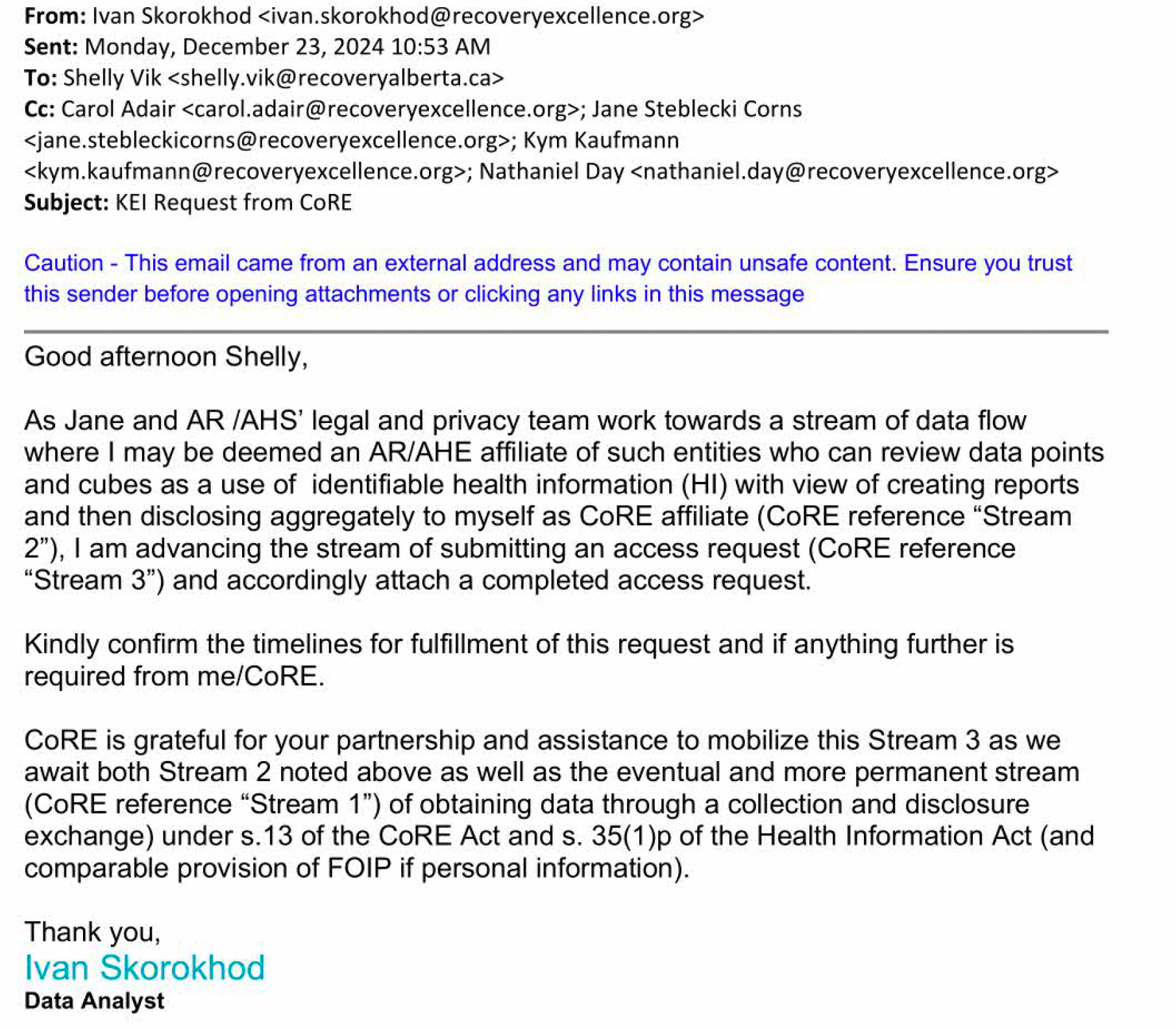
Just three days later, the CoRE followed through on this commitment. In an email copying senior Recovery Alberta and CoRE staff, the analyst asked to create "a stream of data flow" that would include "identifiable health information (HI)."
The analyst, who had submitted the original Information Request on behalf of CoRE CEO Kym Kaufmann, emphasized that the personally identifying health information 'data stream' would become a permanent channel, as permitted through the CoRE Act.
Hardcastle finds this detail troubling. "There's a whole slew of factors that necessitate a lot more thoughtfulness than seems to maybe have gone into that," she told Drug Data Decoded. "They're saying, 'We need this information,' and then, three days later, 'we need more information' ... But this is not something they've done before. It's not something other places are doing."
The Canadian Centre of Recovery Excellence Act (CoRE Act) governs the organization's activities and was passed into law on May 16, 2024. It provides that the CoRE may "collect, directly or indirectly, use and disclose information, including personal information and individually identifying health information... without the consent of the individual who is the subject of the information" for the purpose of "facilitating … provision of services."
The Health Information Act (HIA) governs the management of health records, with many provisions to secure personally identifying records from undue collection, use, or disclosure. For example, the HIA requires that an individual be notified if their personal data are being collected, used or shared. It also allows for data 'custodians' – those charged with collecting and protecting sensitive health information – to refuse to disclose data if it could put a person in danger.
The CoRE Act contains neither of these safeguards. People whose individually identifying data are used by the government are not necessarily aware of this fact, and when a request for data is sent by staff at the CoRE, service providers have no option to refuse.
Hardcastle has concerns about the data "potentially being used in a way that profiles certain people or links to criminal law data sets or health data sets [in a way that could] criminalize certain groups or certain health behaviours... We're not talking about something innocuous. We're potentially targeting people for criminalization or involuntary treatment. The consequences are significant."
The Compassionate Intervention Act was given royal assent on May 15, 2025. "We're obviously stripping away people's Charter rights to 'compassionately intervene' in their lives and to hospitalize and treat them without consent," says Hardcastle. She wonders how the government's collection and use of identified health information might "expand the tentacles of that Compassionate Intervention Act. Is that data going to be used to... identify people that may, in their view, require intervention?"
On February 17, Drug Data Decoded asked senior leadership at the CoRE if data about people who use drugs that were collected by the CoRE could be used to place people under Compassionate Intervention Act treatment orders. The CoRE responded on February 27 that it had no comment on the matter.
But, insists Hardcastle, "even if none of these bad things transpire, if it comes to be public knowledge that [personal] information about addiction treatment is being shared... I would be concerned that individuals don't seek treatment on their own or avoid particular services or treatments." She worries that this could manufacture a justification for medical detainment, whereby "if people are not getting treatment voluntarily, that then exposes them to things like compassionate intervention."
We're not talking about something innocuous. We're potentially targeting them for criminalization or involuntary treatment. The consequences are significant.
-Dr. Lorian Hardcastle

"We know from the US context what a disaster for-profit delivery of recovery services looks like," says Hardcastle, and wonders what opportunities private companies might access as a result of these new 'data streams.'
Her concerns are well founded. Drug Data Decoded previously reported that collection of personal health information through the My Recovery Plan app, owned by Last Door Recovery Society, was done without informed consent. Later reporting noted that people who use drugs were being coerced into providing their health information to the app, which could be used to entrap them in involuntary treatment under the Compassionate Intervention Act.
In August 2025, soon after Drug Data Decoded reported that the Auditor General was investigating My Recovery Plan, Minister of Mental Health and Addiction Rick Wilson quietly confirmed that the app was being decommissioned. In a November legislative committee, Deputy Minister Evan Romanow attempted to clarify that "My Recovery Plan, just to be very clear, is not being abandoned. The platform is being scaled out."
Asked by MLA Janet Eremenko what he meant by "scaled out," Romanow explained that the Ministry would "leverage the innovative My Recovery Plan platform to be able to mature the research evaluation process and expand a digital tool to deal with all of the service providers."
This "maturing" of the research evaluation process appears to have been initiated almost year before Romanow's legislative appearance, as the CoRE sought access to the personal health records of thousands of people who had unwittingly uploaded their data to My Recovery Plan.
Hardcastle sees other issues raised by this wave of data privatization. She wants to know what other services companies could market to people who use drugs. "What are these private entities planning on selling them to convince them that after they leave this government-paid 'compassionate intervention' period, they're at high risk and 'here's what we'd like to sell you?'" she asks.
"The Health Information Act was written at a time when there were still paper medical charts," says Hardcastle. "And now you don't have this bright distinction [between public and commercial services]. As we've privatized health service delivery, you now have these entities that are no longer one or the other."
Hardcastle also emphasizes that the government has acknowledged it's time to review health privacy legislation, so they should throttle back sharing sensitive information. "Obviously, there have to be exceptions to those [privacy] principles," she says, explaining that system operation requires some data sharing. "But," she continues, "they're meant to be exceptions, not the rule. Your family doctor isn't going, 'here, let's see all the information I could disclose.' No – it's only if needed."
Hardcastle is skeptical that the legislation will get the revamping it needs if that could undermine the Alberta government's agenda. "This is a government that gets an idea in their head, does limited expert consultation... and just forges ahead with it. We've seen the same thing with the private delivery of surgical services," she says.
In that case, Hardcastle notes, "everyone was screaming from the rooftops: 'What about conflicts of interest?'" The fallout of that continues to be significant, with hundreds of millions of dollars evaporating while people wait longer than ever for surgeries.
"If their purpose is evaluating the effectiveness of these programs, planning for future resources needed, understanding who's using these programs – to me, those are legitimate objectives of this entity. But individually identify? What are you doing with that data? Even if the answer is nothing nefarious, then if you don't need it, you shouldn't have it."
As ever, it appears that people who use drugs in Alberta are being used as the test case for accelerated health care privatization. Under the guise of 'research' – poorly executed and lousy with conflicts of interest – the government has given itself the power to "collect, use, and disclose" those data however it sees fit, so long as it falls within the purview of service delivery.
And as the government erases the "bright distinction" between public and private service delivery, those data appear likely to continue falling into private hands.
UPDATE (March 29, 2026, 08:18 MST): On March 17, Drug Data Decoded received a response to questions sent to the Centre of Recovery Excellence on February 17. The CoRE responded to three of the seventeen questions, though eleven of them pertained directly to CoRE staff (in some cases during their employment by Recovery Alberta, another entity of the Ministry of Mental Health and Addiction). Here are the CoRE responses:
"Question 15. On December 23, 2024, Ivan Skorokhod (CoRE) asked Dr. Vik to begin establishing a data stream for CoRE to access personally identifying health information. Was this request fulfilled? If so, who at the CoRE currently has access to identifiable health information?
Answer: No, the request was not fulfilled. CoRE does not have any identifying information on its premises. CoRE is in the process of building a secure analytic environment to hold such information and therefore until then, the organization cannot hold any identifying information.
Question 16. A March 3, 2025, email from Dr. Vik to staff at the Red Deer OPS showed a list of measurements to be collected in a “measurement plan” due last June. The listed measurements included pregnancy and a series of medical conditions. Are data concerning pregnancies and medical conditions among SCS clients being analyzed by the Canadian Centre of Recovery Excellence? If so, who has access? Are these data individually identifying?
Answer: Data concerning pregnancies and medical conditions amoung [sic] SCS clients is not being analyzed by CoRE at this time. As stated above, CoRE is not in a position in its current state to hold any identifying information.
Question 17. Section 13(4) of the Canadian Centre of Recovery Excellence Act provides that "The Centre may collect, directly or indirectly, use and disclose information, including personal information and individually identifying health information.” Is there any possibility that health information obtained by the CoRE could be used to issue Orders under the Compassionate Intervention Act?
Answer: CoRE does not have any identifying information on its premises; therefore, these types of questions should be directed to the Office of the Compassionate Intervention Commissioner."
Drug Data Decoded maintains that the research published by the Centre of Recovery Excellence contains personally identifying information, therefore indicating that the Centre does indeed hold or has held personally identifying information on its premises. /End of update
Documents obtained through freedom of information used in this report are available in Part 1 and Part 2 of "How Recovery Alberta facilitated consumption site closures."
An early version of this story was shared with Paid subscribers on March 11.
Drug Data Decoded provides analysis using news sources, publicly available data sets and freedom of information submissions, from which the author draws reasonable opinions. The author is not a journalist.
This content is not available for AI training. All rights reserved.



