
"Inaccurate data": How Recovery Alberta officials facilitated consumption site closures (Pt 2)
Selective data sharing by some of Alberta's top health officials may backstop plausible deniability for government negligence in closing sites – with impacts all the way to Ontario.

This is Part 2 of a series. To revisit Part 1, click here.
In early 2025, a legal battle was underway over the Ontario government's closure of supervised consumption services. To refute the plaintiffs' experts asserting the positive health outcomes of supervised consumption services, Ontario enlisted its own experts to testify in favour of closing the sites.
Among them was Dr. Nathaniel Day, Chief Scientific Officer at the Alberta government's Centre of Recovery Excellence (CoRE) and longtime proponent of the government's 'recovery-oriented system of care.'
In his legal affidavit, Day described data held internally by Recovery Alberta showing that supervised consumption service utilization is not associated with visits to the emergency department, physician services, detox or residential rehab.
However, new documents obtained by Drug Data Decoded show that Day's affidavit failed to mention some key findings.
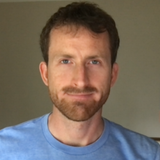
According to the Recovery Alberta data, which were being prepared as a "Retrospective Cohort Study" manuscript at the time, hospitalizations for "substance use or poisoning" among people who regularly attend consumption sites in Alberta are half as frequent and half as long in duration than among less frequent site visitors. (It is unclear why the study combines poisonings with outcomes that are less relevant to supervised consumption, such as psychosis.)
The unpublished study also reveals that supervised consumption site clients show two- to four-times higher initiation of opioid agonist treatments (OAT), such as methadone and buprenorphine, than non-clients who use drugs. Despite overseeing OAT virtual prescribing across Alberta and promoting OAT in his affidavit, Day also omitted these data from his affidavit.
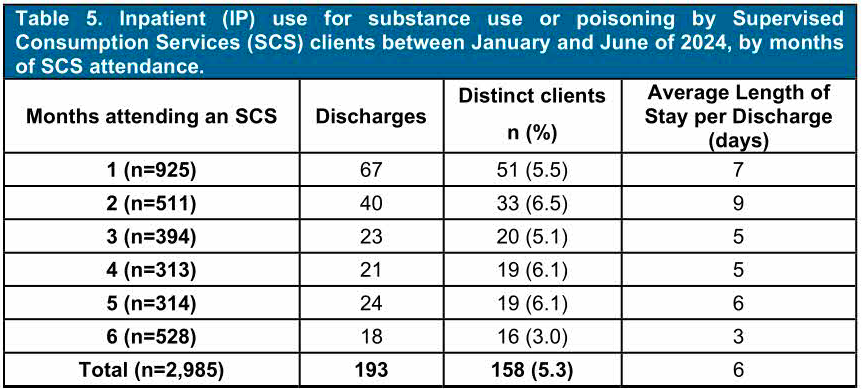
Day's affidavit was sworn on January 24, 2025. Four days before that, he asked the Recovery Alberta study's author, Dr. Shelly Vik, if he could "join the project team to help." Vik's response praised "earlier reviews" Day had provided to the study.
Reduced hospitalizations of regular supervised consumption site clients reinforce the findings of a landmark study that Day also dismissed in his affidavit.
That study compared drug poisoning deaths in Toronto neighbourhoods with and without supervised consumption sites. Its key finding was that neighbourhoods with a supervised consumption site had two-thirds fewer drug toxicity deaths in the study period versus neighbourhoods without sites.
In his affidavit, Day wrote that he found it "shocking” and “astonishing” that researchers would link lower drug toxicity deaths during this period to consumption sites in Toronto, because it coincided with a province-wide reduction in drug toxicity deaths.
Day leaned on the truism that 'correlation is not causation,' mischaracterizing the Toronto study as a simple correlation analysis. The study did correlate variables as part of its approach, but it also applied a wide variety of statistical tests while accounting for many confounding factors – including change from before the sites opened to after. It was published in a top-ranked public health journal.
On February 23, Day was asked to explain his omission of the hospitalization data and mischaracterization of the Toronto study in his affidavit. He did not respond.
Day also served as an expert witness for the Alberta government in Ophelia Black's successful 2023 injunction to protect her access to regulated hydromorphone, which the government is currently trying to overturn.

A study in scarlet
In 2024, Vik and her team began mobilizing personal health numbers collected at supervised consumption sites for the Retrospective Cohort Study. They soon realized that their analysis was built on a deeply flawed assumption: while people who use supervised consumption sites are identifiable when they choose to provide a personal health number, personal health numbers are not consistently collected. Meanwhile, as discussed in Part 1, site clients appear to routinely exchange personal health numbers and continue to supply those of people who have died, to gain access to sites.
Despite it being impossible to say with certainty who is or is not a user of supervised consumption services, the Recovery Alberta study data are entirely dependent on getting this right.
The study also fails to analyze outcomes related to the number of consumption site visits per person, despite these data being captured, and Recovery Alberta did not explain when asked.
An email sent by Vik to high-level Ministry and Recovery Alberta officials on January 14, 2025 suggested that the study is still planned for peer review and publication, but which data will be included in the study and how they will be interpreted by the authors remains unclear. Recovery Alberta officials did not respond to questions on the matter.
The cohort analysis created internal strife around January 10, 2025 – two weeks before Dr. Day signed his affidavit – when the Canadian Research Initiative in Substance Matters (CRISM) research group requested consumption site user data for an independent study. Heavily redacted emails suggest panic in the Ministry, as officials insisted Recovery Alberta protect the data from "external" parties. The Ministry, it seems, did not want the Cohort analysis getting out.
![From: Steven Clelland. To: Kenton Puttick, Shelly Vik, Tuxephoni Winsor. Date: Friday, Januayr 10, 2025. Subject: SCS Cohort Analysis. Body of email: One last message Kenton – to your question / comment back to me. When I read such firm messaging from Tyler [Marshall] specific to MHA approval required beyond those who worked on the analyses – why I note this as several of us were not in the throws of the work itself. It is the tone and directive messaging if it is interpreted literally eg Kerry would not have been involved and he is RA staff as is Nick for example. I did not think you would interp this way – so I use this to be obvious. :) Captain obvious today. Think we are all aligned and on same page – and I am happy to connect with Tyler or any and all of us on this topic – never harm to be clear on intent as we are all on the same team in the end. TGIF. Take care.](https://drugdatadecoded.ca/content/images/2026/02/Screenshot-2026-02-14-at-4.38.31---PM.png)
In another timing coincidence, the supervised consumption site Cohort Study data were formally reported to the Ministry on September 27, 2024, three days after it publicly announced the closure of the Red Deer consumption site the next spring.
Carolyn Corrigal, executive director at Turning Point Society, which ran the Red Deer consumption site until 2023, told Drug Data Decoded she does not think these data would have changed the Ministry's mind in any case. "Plans for site closure seem to have occurred before access to sufficient data, so it doesn't seem to be what informs these decisions," she said. However, she still believes that accurate data is critical for advocacy and to "more effectively inform agency responses."
Red Deer, revisited
"I hope this issue can be resolved quickly, so we don't continue to submit inaccurate data to the government of Alberta," the Red Deer consumption site manager pleaded to senior Recovery Alberta officials twice in January and February 2024. The vote was upcoming by the Red Deer city council that would seal the fate of the consumption site.
The data in question concerned supervised consumption site usage statistics and drug poisonings that were being reported by Recovery Alberta to the Ministry of Mental Health and Addiction.
"Have the reports been fixed? The numbers submitted to GOA that were inaccurate are being used as a way to close the [consumption site] on Monday," the manager insisted again.
Another staff member chimed in to the email thread, "Unfortunately, we have our city council meeting next Monday and they may be making a decision on the future of our overdose prevention site utilizing data that potentially does not reflect the accurate number of visits since AHS assumed operations. Is there any way this [correction] can be expedited?"
The Red Deer consumption site manager's requests to correct the data were refused by Recovery Alberta Director of Knowledge, Evidence & Innovation Shelly Vik, who told the manager and others, "we do not want to have to go back to [the Ministry] with more corrections... As well – it does not sound like the main numbers (visits and distinct individuals) are problematic... the main revisions are expected to be for the adverse events, which are not at issue here."
The Ministry and Recovery Alberta were asked on February 17 if corrected data on adverse events or visits were ever shared with the Ministry. They did not respond.

Drug data distorted
As the Red Deer consumption site closure proceeded in early 2025, the Ministry was turning its gaze to the site in Lethbridge.
On February 3, 2025, the Ministry asked Recovery Alberta officials to explain the discrepancy between the Total Visits to each supervised consumption site and the number of visits that had "intention," which it defined as consumption events or referrals to other services. The Lethbridge consumption site was flagged by the Ministry, as around half of visits to the site lacked "intention" from 2022 to 2024.
In this implicit accusation, the Ministry was ignoring its own closure of the Lethbridge ARCHES site that operated until 2020. Equipped with 13 injection booths and two inhalation rooms, that site had been the busiest in the country. The modular trailer that replaced it, run by Alberta Health Services, had just three injection booths, no inhalation room, and the total capacity was five people.
As a result, most Lethbridge consumption site visitors now access sterile supplies to use elsewhere, rather than consuming onsite. Several months before the Ministry's question, Recovery Alberta knowledge and evaluations director Shelly Vik had asked Lethbridge consumption site staff, "Can you tell me why there are so many visits that are not consumption events?"
The consumption site staff replied:
"...the summer trend of people wanting to stay outside, staying in encampments or going to stay/work out of town... leads to a lot of people coming to quickly pick up harm reduction supplies and head on their way.
A second factor which compounds this trend is the Lethbridge Wellness Shelter (where we are normally parked right in front of) is undergoing construction and expansions therefore a lot of the clients are being dispersed from encampments by the city of Lethbridge and are having a harder time making it to our temporary location.
...our consumption numbers are consistently lower than other sites [because] the Lethbridge [consumption site] has the smallest capacity of all the sites, we have 3 consumption booths, where we can only facilitate IV injections (We do not offer smoking services on board) and have a limitation of only 5 clients on board at a time due to fire code regulations."
This explanation, which also raised encampment evictions as a contribution factor, does not appear to have been communicated to the Ministry by Recovery Alberta, and neither public body responded when asked twice whether it was shared internally.
Instead, Vik told the Ministry, "Unfortunately, I am not surprised... Regarding Lethbridge, this site will report more than one visit if person [sic] comes in and uses drugs, then also picks up a naloxone kit (for example)... Thus, we feel it most accurate to look at ONLY consumption visits."
But it was not only the loss of the inhalation site and four-fold reduction of booths at the Lethbridge site that drove down site visitors. Following the outbreak of the COVID pandemic, visits to supervised consumption sites appeared to plummet across Alberta. In Calgary, which had nearly 1,200 unique visitors per month in 2020, unique visitors dropped to around 500, where they have remained since – in the official reports.
But internal correspondence from March 26, 2025 suggests that site visitors have been under-counted by as much as three-quarters, possibly because of a data glitch following the provincial transition to the Connect Care database.
Drug Data Decoded asked a worker who uses the reporting system to untangle the data. On condition on anonymity, they said the data Recovery Alberta officials were sharing show that around 2,100 people were visiting Safeworks each month from November 2024 to February 2025 to consume drugs (figure below, teal) or access safe use supplies or other services (figure below, purple).
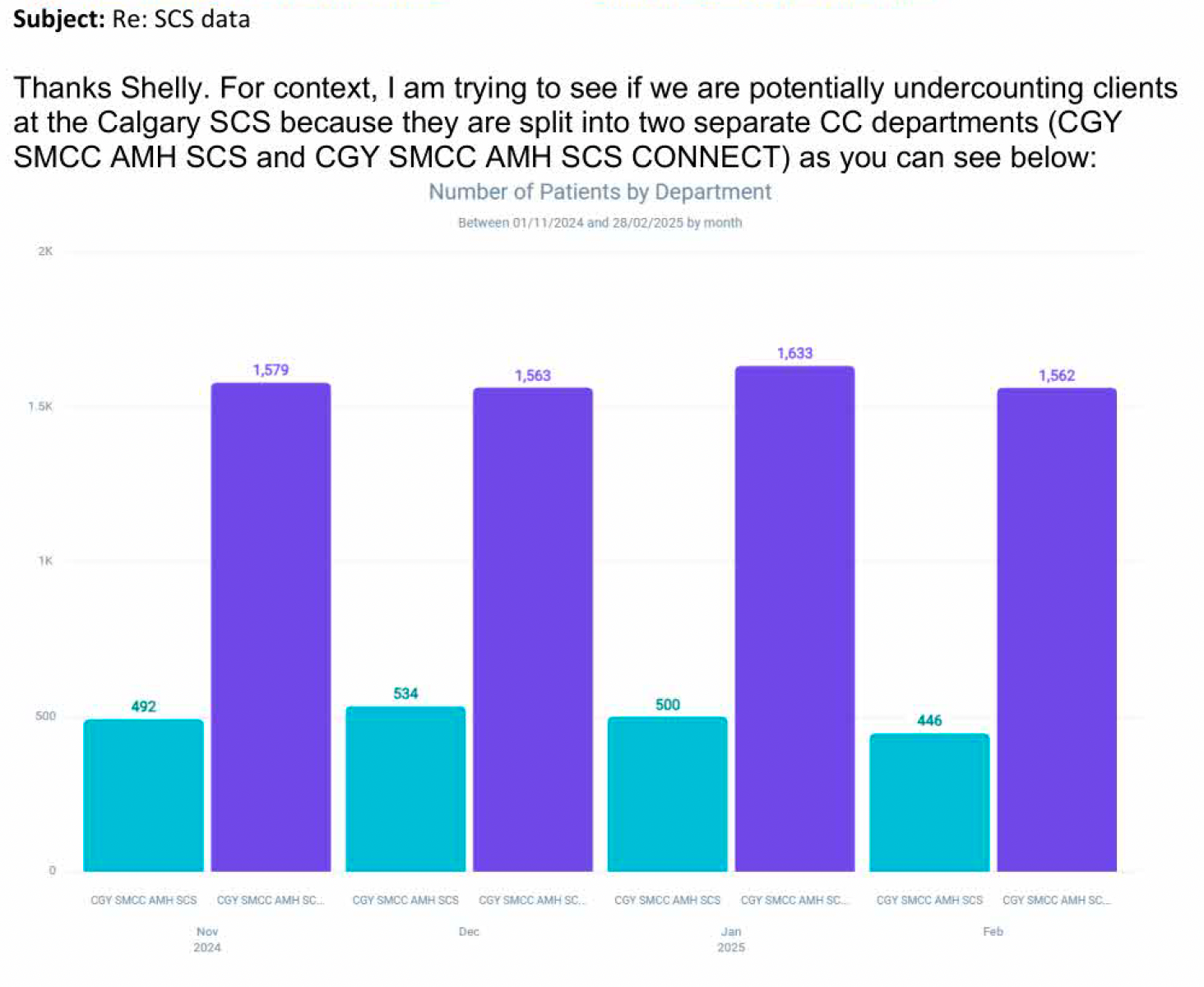
But the Recovery Alberta analyst reporting these data to the Ministry suggested that the values reported publicly are "historically consistent" with previous monthly site visitor counts of around 500 – ignoring the pre-COVID period, when monthly visitor counts were closer to 1,200.
In response, Vik confirmed her initial worry with the analysis team, suggesting "the other department is currently missed, and has been historically – it would be good to know where they were storing the data from the other department pre-Connect Care."
Recovery Alberta and the Ministry were asked which of these counts is accurate for total monthly site visitors and total unique monthly site visitors. They were also asked if Calgary Safeworks receives in excess of 2,000 site visitors per month, most of whom do not show up in the public dashboard. They did not respond.
As Drug Data Decoded reported in June 2025, the Alberta government failed to backstop funding for sterile drug consumption supplies as demand skyrocketed, forcing distribution nodes to ration supplies and eventually halt distribution. The newly obtained documents show multiple requests from Recovery Alberta executive leadership to managers to identify cost-saving measures within the organization throughout 2024.
In short: Visits to supervised consumption services are deflated through selective data collection, by cuts to frontline services, and by aggressive encampment policy. Together, these manufacture the Ministry's justification for criticism of services, and incomplete data shared by senior Recovery Alberta officials appears to backstop plausible deniability for the Ministry's negligence in closing sites.
The public record has never been corrected on these matters. The government's online dashboard, which it has described as “the most transparent data reporting system in North America" for drug toxicity, maintains these records as if no glitches were discovered by Recovery Alberta.
Morgan Magnuson is a nurse and PhD candidate at the University of Lethbridge who has studied the impacts of closing the country's busiest consumption site in that city. She explained to Drug Data Decoded that the Alberta government appears to be "using a strategy of suppressing utilization or finding reasons to accuse sites of not being utilized enough, to create justification for closing them."
Another apparent mechanism to suppress visitor counts at sites is by restricting street outreach activities. Many sites carry out such activities primarily because most overdoses occur following inhalation drug use. However, Alberta's only supervised inhalation site, in Lethbridge, was closed by the government in 2020. This means more drug use – and drug poisonings – in public spaces.
On March 24, 2025, Vik asked one of her staff to send her "the clause from the [consumption site] grants that specifies use of funds for other purposes." After that did not produce what she was seeking, she clarified, “I was looking for something that states the objective of the [consumption site], and indications funds can be used for things like outreach. A meeting would be great."
This was not resolved in the released emails. Several days later, Vik took on a new role as Executive Director of Evaluation and Research at the Canadian Centre of Recovery Excellence (CoRE).
Around this time, Bowline Health, a subsidiary of the private government-linked company ROSC Solutions Group (RSG), was taking a more active role in contracted outreach activities. This included in the shelter near the Red Deer consumption site, which was formally closed on March 31, 2025, in 'navigation centres' where unhoused encampment evictees were sent by police, and in emergency departments across Calgary.
Erasing the soft overdose
Drug poisonings that do not require the use of naloxone or oxygen are sometimes referred to as "soft" overdoses. A frequent response in these situations is to monitor breathing and heart rates, while attempting to maintain communication with the patient – verbal, hand squeezing, or otherwise.
Magnuson describes a drug poisoning as a "declining state, so if you catch it early, you can manage it with minimal intervention. But if you don't, people can go into a full-blown overdose."
Soft overdoses are recorded in the Ministry's dashboard as adverse events "requiring supportive care only," and these were previously included within the tally of total adverse events. The documents reveal that while the Province and Red Deer city council were planning the overdose prevention site closure in February 2024, Vik began questioning whether soft overdoses should be included in the adverse event tally.
Magnuson says this demonstrates a "poor understanding" of drug poisoning by senior officials. In a medical response, she says, "you always choose the path of least intervention, because the more interventions you give, the more likely your intervention could have an adverse impact."
"We don't go to C-sections immediately when people are struggling with birth, right? You start with the least amount of care possible."
Morgan Magnuson, University of Lethbridge
By March 3, 2025, Vik was bringing this matter to top executives at Recovery Alberta, including Chief Operating Officer Thomas Mountain: "The 'supportive care' events are provided very inconsistently by sites, and it is a very subjective measure (e.g., 'speaking loudly,' sternal rubs). I have asked that they remove this from the Mental Health Services Protection Act, as the sites cannot be compared at all with this measure."
The result of removing soft overdoses from the 'adverse event' tally would be a reduction in the apparent number of adverse events under supervised consumption.
Magnuson suggests that omitting less complex poisonings from the count is "one way that [the government] could suppress data showing the effectiveness of supervised consumption."
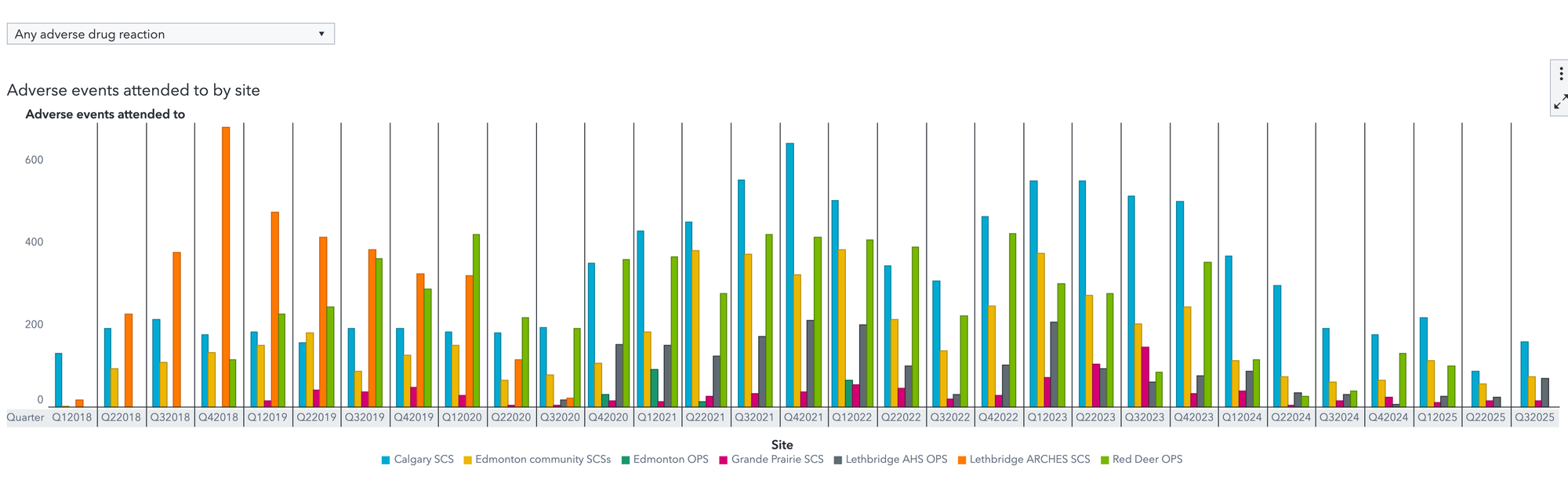
Drug Data Decoded determined that soft overdoses were removed from the Calgary Safeworks tally of adverse events in the third quarter of 2025, without past data being similarly adjusted. Therefore, the current presentation of the data could mislead trends by artificially inflating declines in adverse events. (In previous quarters, total adverse events equalled the sum of events where oxygen was administered, EMS was called, and 'supportive care only' was given. For example, Calgary Safeworks, below in blue, should show 200 adverse events for Q3 2025, not 160.)
The Ministry was asked if this reporting change related to internal advocacy by Recovery Alberta officials. The Ministry did not respond.
Magnuson feels all of this fits a pattern. "It shows the ways the Province misrepresents data in their overall goal," she says, "which is to defund harm reduction and move to this system of recovery-oriented care. We know that will not meet the needs of everyone using substances, because it misses people who don't need or want treatment."
Carolyn Corrigal and her team at Turning Point are watching the Alberta government's agenda play out in the streets of Red Deer. She says the data show "tremendous increases in community opioid poisonings on the doorsteps and bathrooms of downtown businesses, in other frontline agencies and to the places people were displaced, such as in the woods." Demand from businesses and residents for overdose response training has risen sharply, "as these emergencies are now occurring in spaces they did not normally occur before."
"It's worth noting," Corrigal finishes, "that upcoming data may not be accurate either, regardless of [government] suppression." As service providers can no longer accurately report what's happening, she says, the community is having to look after their own emergency responses.
UPDATE, March 8, 10:37AM MST: A previous version of this story mistakenly described the Canadian Research Initiative in Substance Matters (CRISM) research group as provincially funded. It is not, and has never been. Drug Data Decoded regrets the error.
Documents used in this story, extending additional files available in Part 1:
An early version of this story was shared with Paid subscribers on February 24.
Drug Data Decoded provides analysis using news sources, publicly available data sets and freedom of information submissions, from which the author draws reasonable opinions. The author is not a journalist.
This content is not available for AI training. All rights reserved.



