
Hippocratic Oathkeepers
With the anti-safe supply propaganda machine now firm-footed in the far-right, why is a small number of doctors feeding its printing press, National Post Opinion?

Thirty-five physicians and nurse practitioners have signed a second open letter titled “Re: Safe Supply and Opioid Agonist Therapy,” which denounces the federal government’s safe opioid supply pilots. The pilots, which operate on a profit-free model with no incentive for increased prescribing, continue to show strong evidence that they reduce drug poisonings while improving public safety.
The letter effectively requests that the federal government curtail safe supply funding and bring the programs under “supervision-only”—a guarantee of clinical revenue flows—while expanding funding for opioid agonist therapy clinics. Unsurprisingly, these are the same type of clinic many of these doctors run as private businesses.
In tandem, National Post columnist Adam Zivo released his latest spin: the doctors who continue to conduct advocacy without first disclosing their financial interests are being victimized for having these interests examined. While it’s within their right to cry foul if they feel unfairly treated, it is also worth pointing out that baseless victimhood narratives are central to the fascist playbook.
Zivo takes it a step further, personally naming Zoë Dodd and me among the ”safer supply advocates [who] want to smear addiction doctors as corrupt simply because they work in, and thus earn a living from, their own field.”
By “a living,” Zivo is referring to the private returns on residential treatment facilities, urine monitoring screening companies, and opioid agonist dispensing businesses that placed many of the Ontario signatories in the top 5% of billing revenues in 2017-18. Back then, even the open letter author Dr. Meldon Kahan spoke out against the outrageous concentration of opioid agonist prescribing revenues in the hands of a few.
Meanwhile, a likely reason for Zivo to target Dodd and me is that he’s spent a year building his career on tirades against safe supply that leaned heavily into these physicians for commentary. Not once did he question their motives or discuss their financial interests in his writing, which was repeatedly amplified by Pierre Poilievre. Anyone in media with even a basic understanding of genocide should carefully scrutinize physicians in any advocacy context where so many lives are at stake. As someone who has endured its paternalism and stigma, Dodd has been outspoken about her views on addiction medicine.
Zivo’s integrity as a commentator is deeply questionable—as a journalist, utterly untenable. Expect him to continue targeting Drug Data Decoded, and expect him to continue amplifying flimsy victimhood narratives.
Medicine is the delivery van of eugenics
Fascism and corporate profiteering work hand in hand in every modern settler-colonial context including Canada. We are watching this in real time as the western military industrial complex is unleashed on Palestine.
But this doesn’t only manifest through military or policing. Medicine has routinely been called upon to legitimize and carry out the political aims of fascism. By the end of the Third Reich, the archetype of fascism, half of all physicians in Germany were members of the Nazi Party—five-fold greater likelihood than the general population. Physicians were also seven times more likely to join the Schutzstaffel (SS). The reasons for this pattern have been explored in depth and include obedience to authority, professional advancement and ideological alignment with beliefs in “Social Darwinism, eugenics, and the social organism as sacred.”
We can boil these down to supremacy, the jet fuel of fascism.
The fact that so many physicians were “early joiners” to the Nazi Party is also telling. According to Haque et al. (2012):
“the systematic planning and actions of physicians greatly contributed to Nazi power and functioning. Most significantly, physicians played an instrumental role in the notorious euthanasia program, ‘Action T4’, through which approximately 275,000 patients judged by physicians as ‘incurably sick’ were killed by starvation, medication, or gassing.”
It is historical fact that physicians as a profession were central to the genocide of 6,000,000 Jews and 5,000,000 Soviet prisoners of war, ethnic Poles, Roma, Serbs, 2SLGBTQQIA people, people who use drugs and people with disabilities, Black people, Jehovah’s Witnesses, and political dissenters.
Post-WWI in Canada, in parallel with Indian Residential Schools and family separation, doctors were permitted to forcibly sterilize Indigenous women and other marginalized groups, with over 1,150 sterilizations of Indigenous women documented in a single decade. The laws allowing forced sterilization were not repealed until the 1970s.
Given this history, as the unregulated drug toxicity crisis can justifiably be framed as a genocide killing more than one million people who use drugs across Turtle Island—disproportionately Indigenous, Black, disabled, 2SLGBTQQIA—it is wise to keep an eye on the ways physicians show up in its politics.
At their core, safe supply programs are anti-genocidal.
Hippocratic Oathkeepers
The crystallization of multiple right-wing movements in response to progressive drug policy should not come as a surprise. Given the marginalized demographics of people most heavily affected by drug poisoning, this a moment to watch how physicians conduct advocacy in its intersecting spaces.
Enter Dr. Lori Regenstreif, a signatory to the new letter. In September 2022, she co-authored a letter to the BC Medical Journal that takes aim at gender-affirming care. Three guest editors sought to educate the authors on transgender health standards of care in a response.
[Update, November 21: In April 2023, Dr. Regenstreif presented at Genspect’s Bigger Picture conference, notable for bringing together leading voices in transphobic academia. She presented on panels covering topics such as “how the concerns of parents have been silenced” and “detransition and post-transition complications” and provided a solo presentation titled “Gender Healthcare Issues that Primary Care Providers need to know about.” Other talks covered “Gender Ideology as a Religion” and “the suite of bills that is “enforcing” gender ideology within the culture and the multiple impacts of these on equality legislation.” American anti-harm reduction advocate and attempted politician Michael Shellenberger gave the keynote at November’s Bigger Picture conference, and his views on trans people were compiled in a recent San Francisco Chronicle opinion piece.]
We’ve discussed the growing alliances among reactionary movements like those forming up against trans rights and harm reduction. These were laid bare when we drew attention from various far-right factions at our Alberta Recovery Conference protest last February. With far-right politicians having taken up these mantles, it’s fair to generalize backlash against harm reduction by those holding significant power as part and parcel with the reactionary politics that appear set to dominate this decade.
And while some of these thirty-five clinicians are no doubt advocating purely for the public interest with no obvious profit motive, even for these, it seems deeply paternalistic and colonial to hold survival data from safe supply programs at their fingertips and still refuse it while their patients—far too many of them Indigenous—succumb to drug poisoning by the dozens.
If their political views align with the far-right, it is unlikely they will be swayed by the evidence on safe supply or by indications of profiteering among the doctors with whom they co-sign these open letters.
As usual, it is activism that will secure progress for policy-marginalized communities.
112-year medical gold rush
Considering the moral stance of these clinicians is critical. Mitigating risks of drug use by teenagers merits care and attention, so long as it does not escalate to moral panic. After all, most of us grew up experimenting with drugs, but things were safer before the age of fentanyl. As it stands, the evidence remains clear that people are not dying from diverted safe supply, including youth. The sweeping majority are dying from unregulated fentanyl. (We will address ‘addiction’ shortly.)
Many of these advocating clinicians have been working long enough to remember how opioid prescribing was done in the 1990s-2000s.
In 1996, Purdue was issued the patent for Oxycontin, which, like heroin in its day, promised to carry no addictive properties. This blew open a new market for prescription opioids to join the SSRI antidepressants such as Prozac that were already widely dispensed, in addition to the benzodiazepines like Valium that were medically popularized in the 60s and the barbiturates before them.
In Canada, these legally prescribed drug classes each stepped in to partially fill the void on vilified substances that were increasingly criminalized from the 1907 Opium Act onward. The psychoactive drug market was brought under strict physician control starting with the 1911 Opium and Narcotic Drug Act.
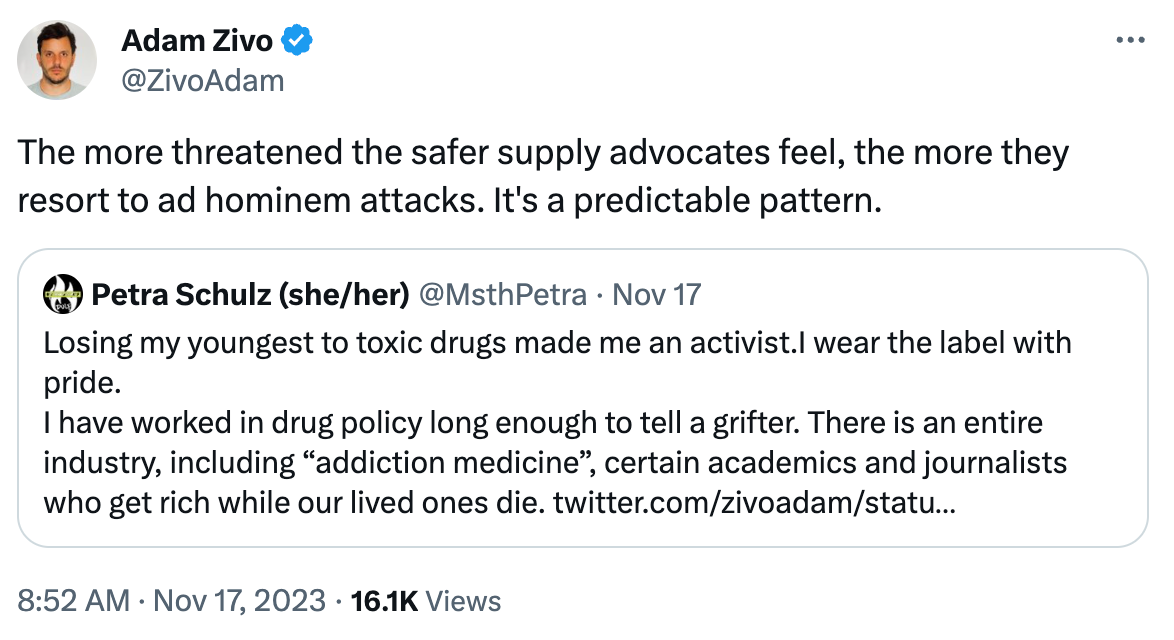
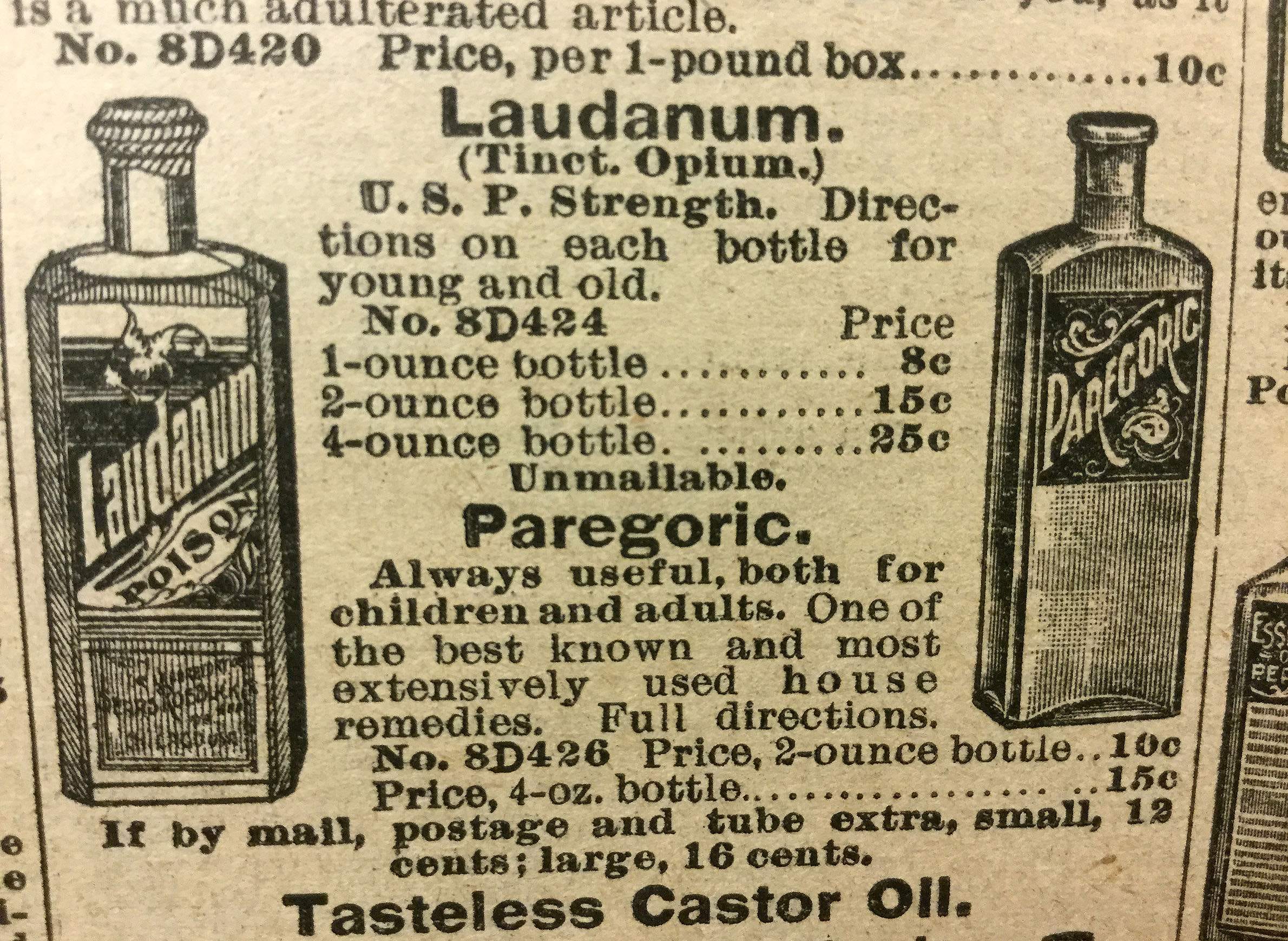
Consider this shift: you could buy tinctures containing heroin, opium, morphine or cocaine a little over a century ago as a consumer product. They weren’t a big deal, they were popular, no illegal market existed, and nobody was dying from accidental poisonings. Since then, we’ve centralized control of these substances into two markets: legal medical suppliers and illegal street suppliers.
The successive waves of wonder pharmaceuticals were painstakingly detailed in The Cult of Pharmacology, a valuable read for anyone interested in this history. Each time a pharmaceutical drug fell out of fashion (often in response to their popularity among marginalized communities), it would be demonized in medical journals and a new one would be pushed into the market with the bold promise of being addiction-free.
Central to The Cult of Pharmacology is a critical question many people fail to grasp: what really is “addiction”? What evidence suggests that drugs hold magical powers to enslave their users after a few experimental uses?
It turns out, there is little evidence that opioids, amphetamines, or even nicotine hold such powers through pharmacological means alone, and the science has supported this since the 1950s. A classic example is the nicotine patch. If cigarette addiction occurs as exposure to nicotine—even chronic exposure over a long period of time—why are nicotine patches so ineffective in ending people’s dependence on cigarette smoking? There is no dose dependence through which you can stack up more nicotine patches to increase ‘absorption’ (a question raised in reference to cigarette additives) and achieve relief from the urge to smoke.
The book details how the science around ‘addiction’ points far more clearly toward people simply not wanting to feel bad, or conversely, wanting to feel good. The behaviours associated with drug use are at least as powerful as anything pharmacological in driving continued use despite harms. Alcohol consumers are familiar with the social urge to drink despite the impending gloom of a hangover. It’s not intentionally destructive and it’s hardly fair to describe continued use as “palliative,” a stigma-laced term that Conrad Black and other right-wing commentators are urging the public to internalize.
This explains why the vast majority of people who undergo “addiction treatment” resume drug use shortly after: drugs provide temporary relief or improvement, and this dynamic isn’t readily altered through institutionalization.
By framing the drug poisoning crisis as one of addiction, certain politicians, physicians and police chiefs reinforce a misplaced understanding of drug use. This is valuable because it deflects the discussion away from equity and supremacy.
And policy follows. In Alberta, we spend at least ten-fold more on residential treatment beds, with no evidence of reducing drug poisoning deaths, than we do on supervised consumption services. Under supervised consumption, where many-fold higher rates of drug use occur, nobody dies. In residential treatment, we know thanks to Progress Report that fatal and near-fatal poisonings are relatively common.
The new pharmaceutical gold rush: treatment
This brings us around to the latest medical-pharmaceutical cash cows: psychedelics and opioid agonists for addiction treatment. Particularly in Alberta, the so-called ‘disease model of addiction’ is firmly established as the central paradigm of our response through propaganda phrases such as “chronic, relapsing disease,” “in the deadly throes of addiction,” and so on. The effect is to minimize public friction as the government opens the addiction market to pharmaceutical and treatment companies. Alberta is exporting this unified model.
We detailed some of Alberta’s policy beneficiaries in Meet the physicians stonewalling safe supply (Part 3). Among them are Dr. Rob Tanguay’s Newly Institute, which conducts psychedelics-based trauma and addiction treatment and Indivior, a company with a checkered legal history that conducts considerable lobbying in Alberta presumably for its flagship opioid medications, Suboxone and Sublocade.
I’ll make it clear that I am very much in favour of the good work that countless health care clinicians carry out with firm dedication to the greatest of human ideals, those who definitively would not have been among the 50% of card-carrying Nazi Party physicians of the Third Reich. Support their efforts by advocating to your local representative for increased harm reduction and regulated substance use support services.
Drug Data Decoded provides analysis on topics concerning the war on drugs using news sources, publicly available data sets and freedom of information submissions, from which the author draws reasonable opinions. The author is not a journalist.




{kind=link}