
Think like a recovery capitalist: Business basics


If exploitation is the driving force of drug prohibition, privatized 'treatment' is the paved road it rolls on.
So, in the spirit of knowing your enemy, a look at the business challenges faced by these organizations.
This two-part series is adapted from a presentation delivered at Community Conversations: Drug Policy Alternatives for Alberta, held in Calgary, AB on April 2, 2024. If you'd like to hold one in your city, drop me a note!
Businesses exist to turn a profit.
Welcome to the world of business! We hope this series helps you on your journey to Dream Big in private addiction treatment.
Profit happens when revenue exceeds expenses. We will focus on revenue, which is equal to sales at a given price. More sales or higher price mean more revenue.
Here in Alberta, the government sets the price on residential addiction treatment, as they tell service providers applying to run the new sites. Here are the per-day rates that each of three 'therapeutic communities' are allowed to charge. It's not clear why the Lethbridge rate is 22% below Red Deer and Gunn, but let's hope it's not coming off the food budget!
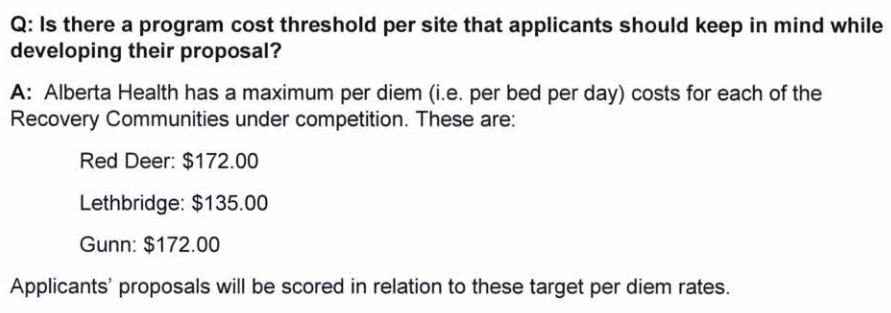
We also know that the Government of Alberta has left a big ol' loophole in its price-fixing. While the government will foot the bill for Alberta residents, out-of-province clients are not included in this scheme. Isn't that a fantastic opportunity?

With sales volume, the problem is to ensure that treatment spaces stay full and that, like a coffee shop full of the laptop class, nobody occupies a space for too long. Each one could be a new customer, after all.
So addiction treatment is kind of like a coffee shop, except in a coffee shop people take drugs to get high and in a treatment facility people take drugs to get better. More seats (or treatment beds) cost more to build but allow for more customers. If you build it big, you need to keep those seats filled. Remember: every coffee drinker (drug user) not in your shop (treatment facility) is lost revenue!
What drives more sales?
Simple: whatever increases the volume of clients. Waiting lists are a good sign that this is working, as long as they don't drive people to find other places to go.

First, sales channels: you need to know who your target clients are and where to find them. This is where tech companies come in, building apps that track people's drug use, service access and 'recovery capital.' Be sure to keep that location data toggled on! Bonus points if you can land the sole-source contract to develop the app and hoard province-wide client data for yourself.
You'll find many customers in the workforce. Workers know how nice it is to unwind after a hard day! But if they say it too loudly, be sure their employer can mandate sobriety and push employees who use substances into your profitable 'return-to-work' treatment program, when they get caught in a urine screen. They always do, with enough well-timed screenings.
Housing is another place you can drive up your client pool. By dangling run-down housing like a rotten carrot on a comedically long stick, you can make certain that basic needs are met only after your treatment profits are earned. If you need a few extra bucks to cover a staff retreat, clear out a whole bunch of people near month's end and keep their sobriety deposits. That makes room for new tenants – and more sobriety deposits!
Be sure to work closely with schools and houseless shelters, which are full of people who aren't always given a chance to advocate for themselves. In fact, segregating youth who use drugs into Recovery High Schools should be a priority for your provincial government to ensure you have reliable revenue, as troubled teens offered abstinence-or-the-street progress into adulthood. Police also make excellent partners!
Without going too deep into vertical integration, let's just say if you're looking to offer counselling services to your customers... forget certified counsellors! They're expensive and fussy about how they operate. So make sure your government doesn't conduct any actual governance of your operation. Consider running a store in your therapeutic community to entice captive customers and employees.

What reduces sales?
Likewise, any factor that reduces the flow of customers into your facility will reduce your sales volume. This is to be avoided at all costs!
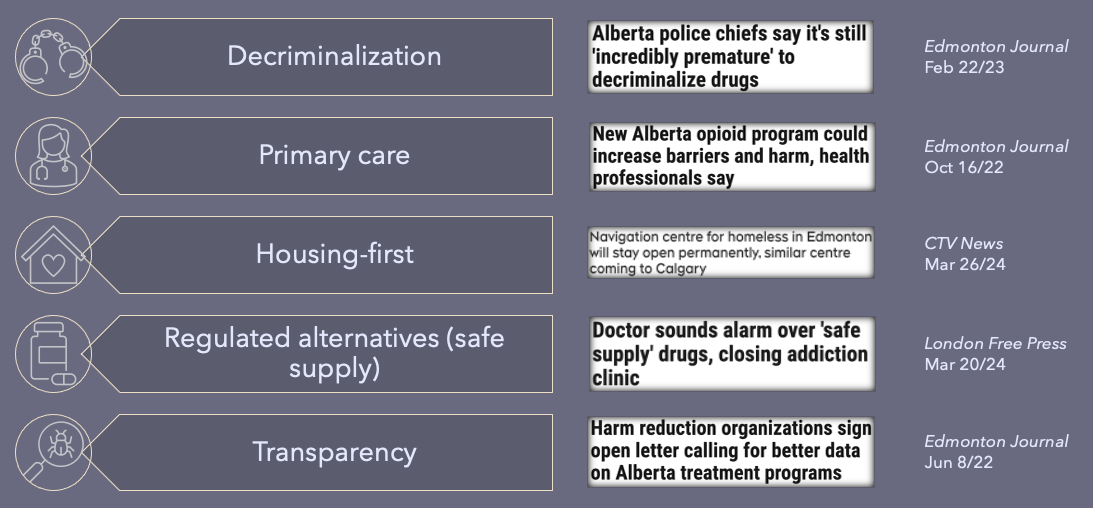
If your government ponders decriminalization, ensure people are pondering what a failure it is before or soon after it starts. Ignore advocates pointing to successes of decriminalization in Argentina, Bolivia, Chile, Colombia, Costa Rica, Croatia, Czechia, Italy, Netherlands, Paraguay, Poland, Portugal, Slovenia, Spain, Switzerland and Uruguay (which never criminalized drugs in the first place). Those backwater countries must have it all wrong – as we know well, treatment or jail are the only rational outcomes for a person who uses drugs. (And don't worry – you haven't lost a customer just because they went to jail. More on this later!)
Family doctors and nurse practitioners who can prescribe drugs should be cut out from between you and your customer. All they do is enable your customer to steer clear of the illegal supply – their quickest route to rock bottom, treatment and salvation. So do what is necessary to wrestle prescribing out of their hands. Alberta's Narcotic Transition Services provided an excellent example to follow, as long we ignore the court challenge the government lost.
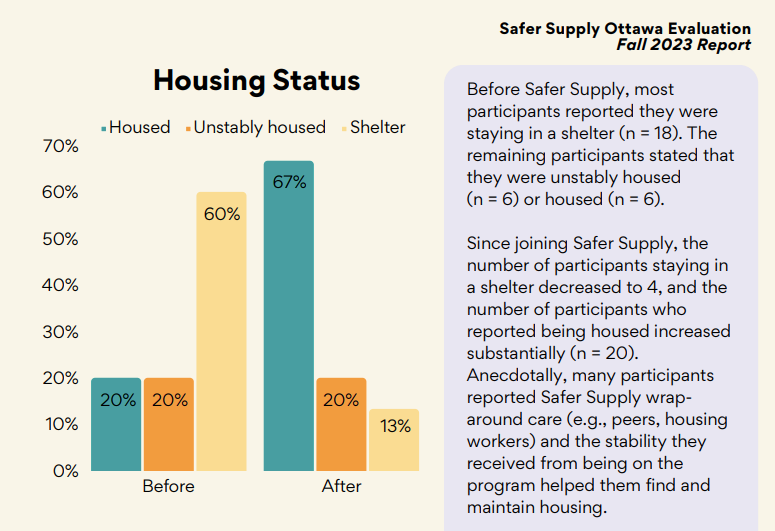
If you let the government start housing-first programs, you can kiss those sobriety deposits goodbye. So make sure to handcuff housing access to satisfactory completion of drug treatment. Remember, we are not out to solve homelessness here – the money's in addiction, a chronic relapsing disease.
Speaking of which, our colleagues in addiction medicine are setting their hair on fire while these godforsaken safe supply programs eat their lunch like a colony of drug use-enabling ants! How is someone supposed to learn they need treatment when they're given the drugs they'd otherwise hustle for? How do we claim our sobriety deposits when their newfound stability helps them maintain housing?
And for crying out loud, do not let these transparency advocates get their foot in the door with 'freedom of information' requests. Bury your data behind private firewalls, and keep it out of the grubby hands of journalists. For all we know, they're funded by Big Pharma, unlike our esteemed addiction medicine colleagues.
Surely there must be exceptions – services that are profitable and help reduce deaths?!
Do try to keep up! Regulated drugs are wildly profitable and help people manage unregulated drug use.
Regulated drugs could be sourced generically, monopolistic business practices could be addressed, lobbying could be brought under control, and public ownership of manufacturing and distribution could minimize conflicts of interest. But we wouldn't want those because they cut into profits!
Regulated mental health services are also both profitable and helpful for people who can afford them. However, be careful not to refer to them under the banner of 'public health' – people might get weird communist ideas.
Note that abstinence-based treatment, unregulated mental health services and services boosting ‘recovery capital’ have no evidence basis for reducing deaths. In fact, residential treatment without medication may even drive deaths higher! But it is profitable, so don't let this little factoid discourage you from achieving your business dreams.
Ok, I've got the basics. How do I crank up my treatment capacity and customer pool?
For the real secrets of the masters, you'll have to drop a few bucks into the subscription signup below.
Just kidding - Drug Data Decoded is always free but we sure do love to hear that tip jar clang! Stay tuned for the second part: we're gonna learn how to build that nice wooden horsey up top.
I'm quite ill and a bit delirious this week. For consistency, the silly tone must continue in Part 2. Please leave feedback in the comments!
Drug Data Decoded provides analysis on topics concerning the war on drugs using news sources, publicly available data sets and freedom of information submissions, from which the author draws reasonable opinions. The author is not a journalist.



